Brain implants pulse hope
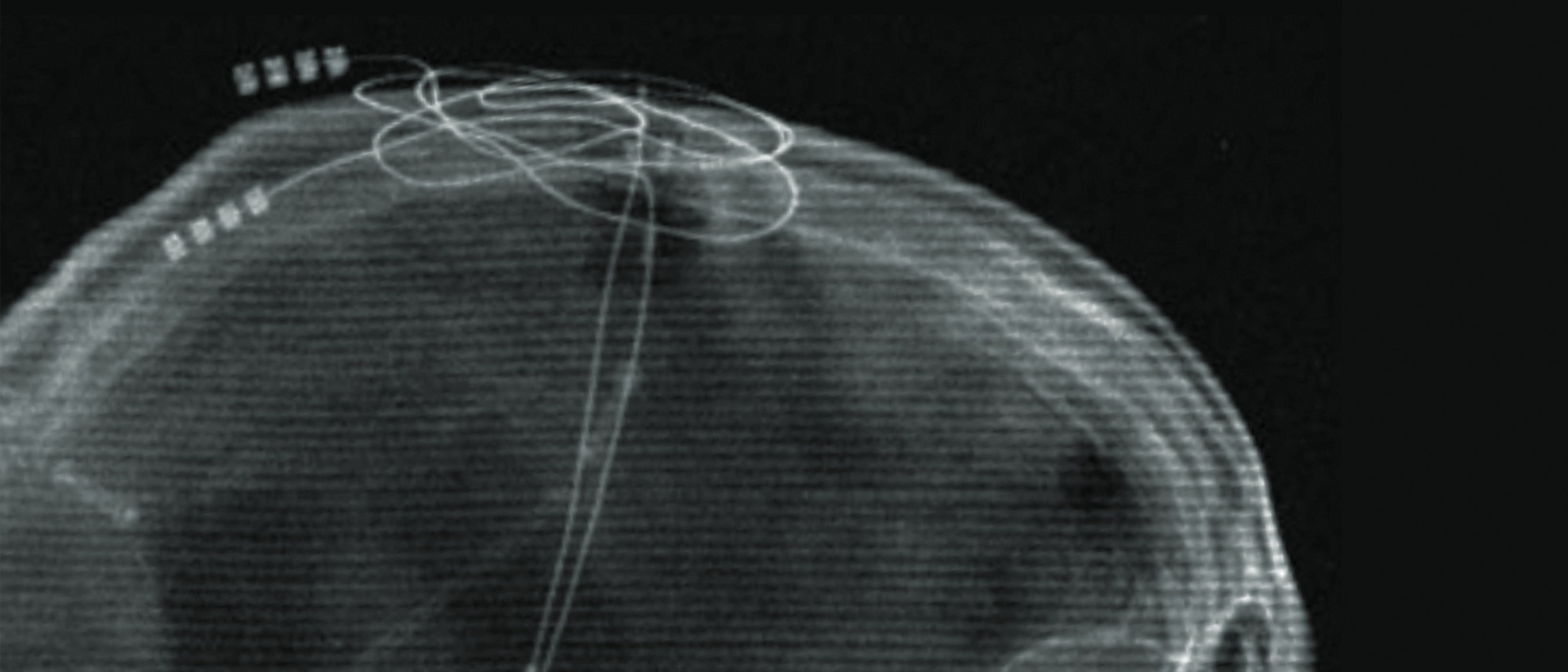
There is a lump in Gina Arata’s chest just below her collarbone. But it’s not the kind to worry about. Inside that lump is a battery and a small computer chip. A wire tunnels under the skin to the back of Arata’s neck and from there to the top of her skull, where it plunges deep into her brain. At the end of the wire, a pair of small electrodes pulse electricity into two kidney-shaped areas near her brain stem. 1
The wire is a lifeline to Arata. Twenty-five years ago, as a college senior, Arata’s car skidded and hit a telephone pole. When she awoke from a coma 14 days later, doctors told her that she was lucky to be alive. Arata had severe trauma that severed circuits in her brain, sure as her car severed that telephone pole.
Arata’s life was never the same. She finished her degree but had to forego law school and move home. She had difficulty concentrating and holding a job. There were mood swings and physical challenges. In social settings, she had trouble reading people. Then, in 2018, Arata’s father was searching the internet for treatments when he came across a call for patients to join a new clinical study. That search brought Arata to Dr. Nicholas Schiff, M.D. ’92, a neurologist and neuroscientist at the Feil Family Brain and Mind Research Institute at Weill Cornell Medicine.
Clinical precision
Dr. Schiff and his collaborator, Dr. Jaimie Henderson, a neurosurgeon at Stanford Medical Center, were looking for patients to test an experimental treatment for cognitive disabilities related to moderate to severe traumatic brain injuries. Arata became Patient 1 in a groundbreaking study. 2 “She was our astronaut,” Dr. Schiff says.
Dr. Henderson surgically implanted electrodes in Arata’s brain and those of five others (though one later dropped out due to an infection), laying claim to a region of their brains known as the central lateral nucleus, part of the thalamus.
The thalamus is, in part, a sort of relay station for four of the body’s five senses — sight, sound, touch and taste. Like a telephone operator, the thalamus handles incoming sensory information and routes it to the cerebral cortex for interpretation. 3 The central lateral nucleus, however, is unique in that it is responsible for regulating frontal areas of the brain needed for cognition. It unites sensory and motor regions of the brain with “thinking” areas of the brain.
“Deep brain stimulation in the central thalamus expands the capacity of the frontal areas of the brain to retain and work with information,” Dr. Schiff explains. “We’re restoring this cognitive processing.”
When these connections are broken, the ability to make logical, physical and emotional sense of the world is broken, too. And Arata’s brain was badly broken. Today, however, six years after implantation, her deep brain stimulator is going strong. Arata says she “feels smart again.”4 She can read and comprehend books, has a better memory, is less irritable, has fewer obsessive-compulsive tics, and enjoys greater muscle control and dexterity.
“It is both brain and motor function that have improved,” she says. “I used to fall down the stairs all the time. And I haven't done it since. When it's off, I can't spread my toes on my left foot. If it's on, I can spread them. It's the weirdest thing ever.”
For Arata’s mother, Marla, a psychologist with a clinical appreciation for all that is going on in her daughter’s brain, the transformation has been astounding. “I’ve had to raise my daughter three times — once as a child, once after the accident, and once again after the implant,” she says. “But the difference between Gina before and after the surgery has been remarkable.”
I think, therefore I am
For Dr. Schiff, the trial was a culmination of years of work on deep brain stimulation, but it was also a return to core interests in the nature of human consciousness and a launchpad toward future work potentially restoring function to patients in minimally conscious states whose awareness and communication abilities are poorer than those in the DBS trial.
His fascination with consciousness had begun as an undergraduate doing historical research at the Montreal Neurological Institute on pioneering neurosurgeon Dr. Wilder Penfield.
“Consciousness wasn’t a popular thing to study,” he recalls, seeing medicine as the best way to pursue the future of this early work.
Dr. Schiff likens the stimulator to a pacemaker for the brain. He explains that deep brain stimulation overrides the underactivated thalamic cells and activates the cells receiving the impulses, restoring the range of their function and — possibly, he stresses — rewiring new pathways. 5 Most importantly, Dr. Schiff has shown that the changes are not temporary. 6
His work is centralized around what he calls the mesocircuit hypothesis of brain injury and recovery that explains how brain circuits are damaged and how they change in response to stimulation. 7 Traumatic brain injury often widely damages the circuits of the brain, and for survivors of this type of damage, there is little hope. But results like Gina Arata’s show that if impaired cells can be kept alive, they can regain substantial function.
‘Still in there’
In 2024, Dr. Schiff and colleagues published what may be their most attention-grabbing study yet. They used fMRI and other brain imaging tools to show that a quarter of the more than 240 unresponsive patients in the study could hear and carry out complex mental tasks following spoken commands, such as “imagine yourself swimming.” The tasks required sustained effort lasting many minutes. One in four patients in the study showed brain activity in the exact regions of the brain over time as healthy people asked the same questions.
“These people, who are thought to be unresponsive, were capable of high-level cognitive tasks,” Dr. Schiff says. That means maybe 100,000 patients in the U.S. are “still in there.”
“The finding was a game-changer,” Dr. Schiff says.
In clinical terms, Dr. Schiff explains that the patients are experiencing cognitive motor dissociation — a disruption between thinking and physical movement. He is now looking to understand what causes these disruptions and, most importantly, whether once identified such persons might regain communication through brain-computer interfaces, like those that have allowed at least one patient with ALS to speak again and those with paralysis to type emails by thought alone.
“One can envision situations in which severely injured patients in minimally conscious state or who have cognitive motor dissociation might receive an effective treatment combination of deep brain stimulation and brain-computer interfaces,” he says.
While Dr. Schiff’s work on deep brain stimulation and on the nuances of cognitive motor dissociation is for now proceeding along parallel paths, he can also foresee a day when those paths converge, and similar deep brain stimulation technologies arise that might help patients recover from coma, stroke and other disorders of consciousness.
Dr. Schiff and colleagues are now focusing on bringing the central thalamic brain stimulation approach that helped Gina Arata through the regulatory process toward an FDA-approved therapy. “If we’re successful,” he says, “a therapy like this could help many people across the world with debilitating traumatic brain injury.”
- Thalamic deep brain stimulation in traumatic brain injury: a phase 1, randomized feasibility study ↩︎
- Subject and Family Perspectives from the Central Thalamic Deep Brain Stimulation for Traumatic Brain Injury Study: Part I ↩︎
- Cleveland Clinic; Thalamus ↩︎
- Subject and Family Perspectives from the Central Thalamic Deep Brain Stimulation for Traumatic Brain Injury Study: Part I ↩︎
- Local changes in network structure contribute to late communication recovery after severe brain injury ↩︎
- Local changes in network structure contribute to late communication recovery after severe brain injury ↩︎
- Recovery of consciousness after brain injury: a mesocircuit hypothesis ↩︎